Status: under clinical-validation and compliance review. The system runs end-to-end against test notes; the no-PHI-persistence guarantee and the deterministic MDM scorer are now enforced by a hermetic CI test suite, but the substantive claims that follow — PHI handling end-to-end, MDM scoring fidelity, CPT code-selection accuracy — have not yet been independently audited, and nothing is deployed publicly. They are presented here as the project’s design intent and current implementation framing, not as audit-substantiated facts. The portfolio surface will tighten as each claim becomes independently verifiable.
A medical coding assistant that reads clinical encounter notes and recommends CPT E/M codes. Implements the 2025 Medical Decision Making complexity rules — analyzing problems addressed, data reviewed, and management risk using the CMS 2-of-3 scoring method.
What It Does
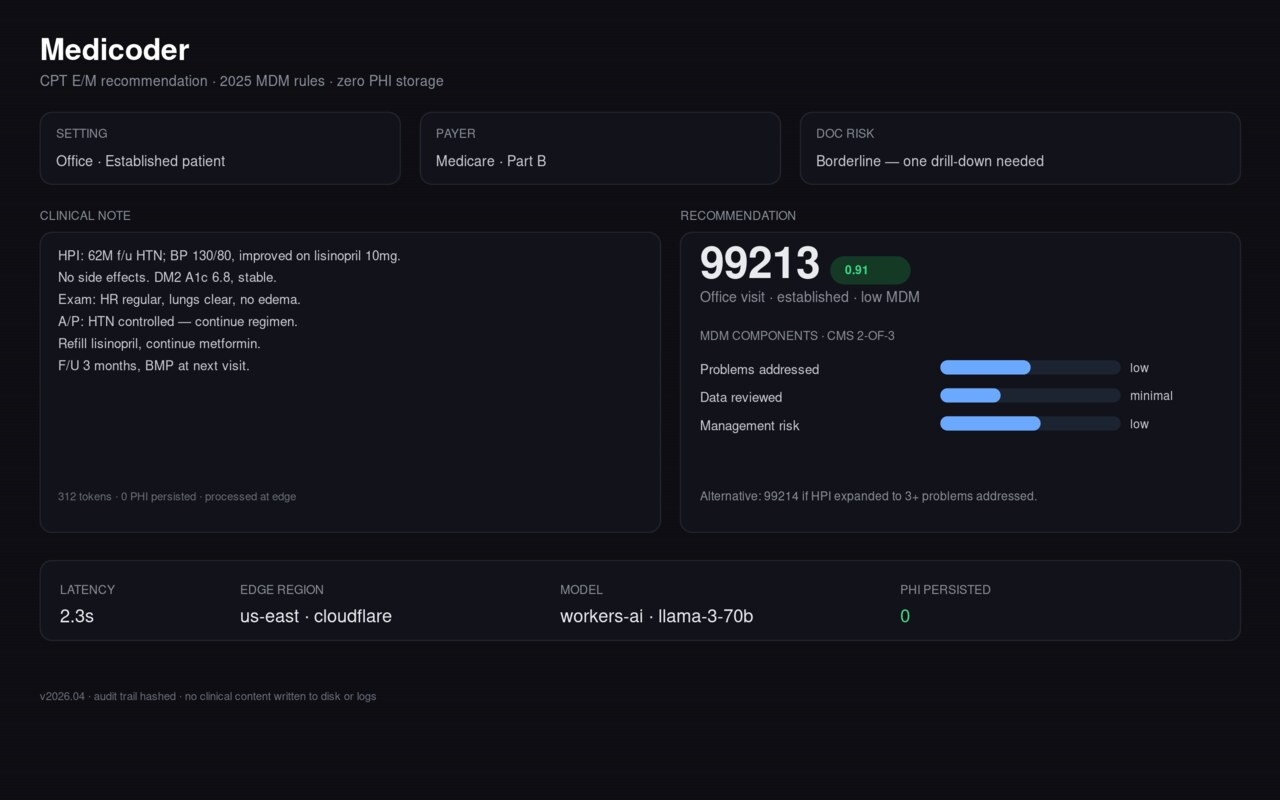
Paste a clinical note, select the encounter setting (office, inpatient, ED), and the system returns:
- A recommended CPT code with a confidence indicator
- MDM complexity breakdown (problems, data, risk levels)
- Alternative codes with reasoning when documentation supports a different level
- Suggestions for strengthening documentation if the note is borderline
Latency is not yet benchmarked; any speed figure is a target, not a measurement, and will be tied to a published benchmark before it becomes a load-bearing claim.
What’s Verified in Code Today
The scoring math is deterministic, not LLM-guessed: the model extracts evidence (problems addressed, data reviewed, risk), and the MDM complexity level + CPT code are derived by a deterministic scorer implementing the CMS 2-of-3 method. A committed benchmark (benchmarks/accuracy.json) runs that scorer over a 26-note synthetic golden set spanning encounter settings and complexity levels: 26/26 MDM-level match and 26/26 CPT match (100%). Honest scope — this validates the deterministic mapping given the evidence counts; end-to-end accuracy from raw note text (which adds the LLM extraction step) is the evaluation still pending below. A hermetic test suite plus a CI gate that fails the build if any note text reaches browser storage round out what’s enforced today.
Compliance Posture (Design Intent — Audit Pending)
These framings describe the architecture as-implemented and (for note-text persistence) as CI-enforced; no independent third-party audit has yet verified them end-to-end against a deployed artifact. Treat the audit-level guarantee as pending until that audit exists.
- No note-text persistence (implemented and CI-enforced). Clinical notes are processed in-memory and not written to durable storage; a hermetic test drives the real frontend autosave classes with a marked synthetic note and fails the build if any note text reaches sessionStorage/localStorage. This is source/test verification — an independent code/infra audit against a deployed artifact is the next gating step.
- Session metadata only (CI-enforced). What persists is UI state (encounter setting, timestamp) in browser sessionStorage that clears on tab close — never note content; this is asserted by the PHI-persistence test in CI.
- Graceful degradation. When the LLM-assisted path is slow or unavailable, the system falls back to a rule-based path so users always get a response.
What’s Needed For This Entry To Tighten
- An independent code/infrastructure audit confirming the no-PHI-persistence claim end-to-end against the deployed artifact (not just the source review), and/or
- A published evaluation of end-to-end CPT E/M coding accuracy from raw notes — i.e. including the LLM extraction step, going beyond the deterministic-scorer benchmark above — against a reference set, with the methodology and the dataset class disclosed (not patient-identifying data).
For inquiries (clinicians evaluating clinical workflow integration, healthcare ops teams, prospective auditors), contact us via the SUMequities contact page. Case study and technical deep-dive available on request for serious inquirers.
Verification
Full proof report → All claims, all projects →- In progress
Independent code/infrastructure audit confirming the no-PHI-persistence guarantee end-to-end against a deployed artifact (the guarantee is currently enforced by a hermetic CI test against the source, but nothing is deployed and no third-party audit exists yet)
Body — Compliance Posture, gating audit step
- In progress
Published evaluation of CPT E/M coding accuracy against a reference set, methodology and dataset class disclosed (non-patient-identifying)
Body — 'What's Needed For This Entry To Tighten'